
Resolving Healthcare's Inordinate Complexity by Transforming Consumer & Provider Experiences

Author
Kiara Bhagwanjee
Complexity is the root cause of healthcare’s costliness, and its inaccessibility. The second order effects — lack of trust, lack of transparency, lack of accountability — beget the industry’s sluggish nature and lackluster progress.
This paper examines the consumer-centered technology solution disrupting healthcare’s status quo, empowering consumers and clinicians to navigate the system with clarity, confidence and ease. The results observed among practices that adopted the technology—outpatient single and multi-specialty private practices, an ambulatory surgical center, and an office-based lab—demonstrate the efficacy and the extensibility of this solution across the market.
The products leveraged here will offer unprecedented data on the industry’s inner workings. Processing up to 40,000 patient profiles per day, verifying the benefits in over 3,600 plans across five specialties—this operating system is designed to withstand the dynamism inherent in assessing real-time consumer out-of-pocket costs, and effectively maintaining information parity across integrated Electronic Health Record (EHR) systems.
Crucially, this solution calculates healthcare’s first upfront, transactable consumer cost-shares. As providers balance the health of their patients and the financial health of their businesses (practices), this consumer-oriented technology guarantees collections, reduces the burden of administrative work, and the likelihood of insurance-based disruptions to care. Upfront eligibility verification and digital patient registration prevent claim denials due to outdated consumer demographics, lapsed insurance coverage or out-of-network providers. This ultimately bolsters trust and certainty. It aligns consumer and provider incentives around a new system in healthcare, affording it the unique opportunity to transform the industry for all.
Complexity is the root cause of healthcare’s costliness, and its inaccessibility. The second order effects — lack of trust, lack of transparency, lack of accountability — beget the industry’s sluggish nature and lackluster progress.
This paper examines the consumer-centered technology solution disrupting healthcare’s status quo, empowering consumers and clinicians to navigate the system with clarity, confidence and ease. The results observed among practices that adopted the technology—outpatient single and multi-specialty private practices, an ambulatory surgical center, and an office-based lab—demonstrate the efficacy and the extensibility of this solution across the market.
The products leveraged here will offer unprecedented data on the industry’s inner workings. Processing up to 40,000 patient profiles per day, verifying the benefits in over 3,600 plans across five specialties—this operating system is designed to withstand the dynamism inherent in assessing real-time consumer out-of-pocket costs, and effectively maintaining information parity across integrated Electronic Health Record (EHR) systems.
Crucially, this solution calculates healthcare’s first upfront, transactable consumer cost-shares. As providers balance the health of their patients and the financial health of their businesses (practices), this consumer-oriented technology guarantees collections, reduces the burden of administrative work, and the likelihood of insurance-based disruptions to care. Upfront eligibility verification and digital patient registration prevent claim denials due to outdated consumer demographics, lapsed insurance coverage or out-of-network providers. This ultimately bolsters trust and certainty. It aligns consumer and provider incentives around a new system in healthcare, affording it the unique opportunity to transform the industry for all.
The U.S. spent nearly the same amount on Medicare and Defense as it did on the billing and insurance work of providing (selling) and paying for (buying) healthcare. That’s the cumulative cost of tasks like acquiring prior authorization, insurance verification, coding, claims submission and re-adjudication, and credentialing with payers.
These administrative costs are known for growing faster than the rate of healthcare spending overall. One estimate suggests they account for 10–14% of revenue at a medical group. As these overhead costs rise for physicians, reimbursement rates and collection rates fall.
Today, some of this administrative work is necessary to parse the unique benefit rules codified in the thousands of public and private plans available to consumers. To quantify this, there are over 6,000 plans listed on HealthCare.gov—that does not include any employer-sponsored plans. Unsurprisingly, nearly 20% of submitted claims culminate in a denial. These incur social and monetary costs to both providers and consumers. Disputing and re-adjudicating denied claims is estimated to cost providers $19 billion per year. More than half of that cost is wasted on denials that payers ultimately overturn.
Consumers receive unexpected bills, which lead them to wrongly villainize providers for additional surprise costs.
This system penalizes practices’ best efforts to comply with the rules, and it offers no means to learn from failed attempts. Sparse data is available about claim denials on employer-sponsored plans, which cover the majority of Americans. Payers don’t publish overall rates of denial, nor their reasons for denial, let alone on a per plan basis. Most of the data available is derived from third party surveys of patients or providers’ experiences with insurance and the Centers for Medicare & Medicaid Services’ assessment of Affordable Care Act Marketplace plans. The lack of transparency keeps insurance users in the dark, and payers from being held accountable. Consumers and practices suffer the consequences—consumers are reluctant to seek care fearing surprise bills while physicians reckon with exorbitant administrative work and inconsistent income streams.
Not only is this complexity costly, it’s punishing. Neither providers nor consumers are empowered to navigate it.
No formal education on billing and coding practices is offered to physicians in training. That is not a shortcoming of medical pedagogy. Billing and coding is a distraction from the core mission of the physician: providing quality care. As such, systems emerged in an effort to streamline that work. EHRs, for instance, provide immense value in the coordination of care. But as the leading digital intervention to help providers surmount the quagmire of billing and insurance administration, EHRs are insufficient. Accurate, real-time eligibility in EHRs is unreliable. Many practices use ancillary verification platforms or contact payers directly. Package selection is similarly inconsistent. Precise pricing for consumer out-of-pocket costs are only available for copays. EHRs do not recognize when plans are primary or secondary, nor do they prompt consumers to review their demographics leaving room for outdated information. All of these errors can lead to claim denials, which prompt a cycle of re-adjudication, angry patients, and lost revenue.
While EHRs alleviate some of the pain points faced by providers, they perpetuate a vicious cycle in healthcare, and uphold processes that no longer serve it. They are rigid and siloed. They draw providers’ attention away from patients. They crash unexpectedly, halting practice operations. They are only relevant as long as the system that currently exists remains in place.
For consumers, health insurance is so confusing it’s estimated that payers and employers spend nearly $5 billion a year helping them understand it. Uncertainty about costs, uncertainty about which providers are in-network, limited appointment availability, these are prevalent barriers to care. Few digital solutions allow consumers to overcome them.
This is a portrait of healthcare today. The processes and technologies that are ubiquitous define consumer and provider experiences, and limit the industry’s ability to evolve.
The U.S. spent nearly the same amount on Medicare and Defense as it did on the billing and insurance work of providing (selling) and paying for (buying) healthcare. That’s the cumulative cost of tasks like acquiring prior authorization, insurance verification, coding, claims submission and re-adjudication, and credentialing with payers.
These administrative costs are known for growing faster than the rate of healthcare spending overall. One estimate suggests they account for 10–14% of revenue at a medical group. As these overhead costs rise for physicians, reimbursement rates and collection rates fall.
Today, some of this administrative work is necessary to parse the unique benefit rules codified in the thousands of public and private plans available to consumers. To quantify this, there are over 6,000 plans listed on HealthCare.gov—that does not include any employer-sponsored plans. Unsurprisingly, nearly 20% of submitted claims culminate in a denial. These incur social and monetary costs to both providers and consumers. Disputing and re-adjudicating denied claims is estimated to cost providers $19 billion per year. More than half of that cost is wasted on denials that payers ultimately overturn.
Consumers receive unexpected bills, which lead them to wrongly villainize providers for additional surprise costs.
This system penalizes practices’ best efforts to comply with the rules, and it offers no means to learn from failed attempts. Sparse data is available about claim denials on employer-sponsored plans, which cover the majority of Americans. Payers don’t publish overall rates of denial, nor their reasons for denial, let alone on a per plan basis. Most of the data available is derived from third party surveys of patients or providers’ experiences with insurance and the Centers for Medicare & Medicaid Services’ assessment of Affordable Care Act Marketplace plans. The lack of transparency keeps insurance users in the dark, and payers from being held accountable. Consumers and practices suffer the consequences—consumers are reluctant to seek care fearing surprise bills while physicians reckon with exorbitant administrative work and inconsistent income streams.
Not only is this complexity costly, it’s punishing. Neither providers nor consumers are empowered to navigate it.
No formal education on billing and coding practices is offered to physicians in training. That is not a shortcoming of medical pedagogy. Billing and coding is a distraction from the core mission of the physician: providing quality care. As such, systems emerged in an effort to streamline that work. EHRs, for instance, provide immense value in the coordination of care. But as the leading digital intervention to help providers surmount the quagmire of billing and insurance administration, EHRs are insufficient. Accurate, real-time eligibility in EHRs is unreliable. Many practices use ancillary verification platforms or contact payers directly. Package selection is similarly inconsistent. Precise pricing for consumer out-of-pocket costs are only available for copays. EHRs do not recognize when plans are primary or secondary, nor do they prompt consumers to review their demographics leaving room for outdated information. All of these errors can lead to claim denials, which prompt a cycle of re-adjudication, angry patients, and lost revenue.
While EHRs alleviate some of the pain points faced by providers, they perpetuate a vicious cycle in healthcare, and uphold processes that no longer serve it. They are rigid and siloed. They draw providers’ attention away from patients. They crash unexpectedly, halting practice operations. They are only relevant as long as the system that currently exists remains in place.
For consumers, health insurance is so confusing it’s estimated that payers and employers spend nearly $5 billion a year helping them understand it. Uncertainty about costs, uncertainty about which providers are in-network, limited appointment availability, these are prevalent barriers to care. Few digital solutions allow consumers to overcome them.
This is a portrait of healthcare today. The processes and technologies that are ubiquitous define consumer and provider experiences, and limit the industry’s ability to evolve.
Healthcare’s modern patient is a consumer. Healthcare’s modern front-door is a landing page online. Crafting a simpler process for consumers in this market elucidates a simpler process for providers too. Superscript’s practice and consumer-facing solutions—the Practice Companion (PC) and Storefront, respectively—deliver this novel experience of healthcare when deployed.
Superscript’s platforms are powered by Healthcare’s First Pricing Protocol, the proprietary technology that makes upfront, transactable consumer cost-shares possible. Both the Storefront and the PC synthesize healthcare’s cumbersome workflows into three clear, simple steps for every treatment, regardless of its complexity: scheduling, payment and intake. This standardization of practice operations, across locations and specialties, removes uncertainty and superfluous work from consumer-clinician interactions.
Consumers shop for healthcare services online with upfront cost-shares. They no longer receive bills in the mail or surprise costs, curbing any further erosion of consumer trust. Instead, they verify their own insurance in advance to access guaranteed, upfront prices. They then browse doctors and treatments, book directly to the practice’s EHR, pay upfront, and complete intake in their native languages before arriving for the appointment.
Administrators instantly verify eligibility and covered services, schedule multi-visit encounters in under 30 seconds, update visit costs in real-time as emergent treatments are rendered, and collect payment all in one tool. This model guarantees consumer cost-shares are paid before the claims cycle begins.
Ultimately, Superscript’s intervention brings healthcare in line with standard market behaviors in consumer facing categories. Consumers are empowered to make informed choices about where they seek care. Practices are empowered to focus on differentiation by providing the best care, and the best experience.
Jamie Hajee Sheriff
- MRN ID to match patient charts
- Insurance verified upfront
- Real-time eligibility checks on demand
- Schedule with real-time availability
- See self-pay & insured cost shares
- Collect payment & digital intake
Healthcare’s modern patient is a consumer. Healthcare’s modern front-door is a landing page online. Crafting a simpler process for consumers in this market elucidates a simpler process for providers too. Superscript’s practice and consumer-facing solutions—the Practice Companion (PC) and Storefront, respectively—deliver this novel experience of healthcare when deployed.
Superscript’s platforms are powered by Healthcare’s First Pricing Protocol, the proprietary technology that makes upfront, transactable consumer cost-shares possible. Both the Storefront and the PC synthesize healthcare’s cumbersome workflows into three clear, simple steps for every treatment, regardless of its complexity: scheduling, payment and intake. This standardization of practice operations, across locations and specialties, removes uncertainty and superfluous work from consumer-clinician interactions.
Consumers shop for healthcare services online with upfront cost-shares. They no longer receive bills in the mail or surprise costs, curbing any further erosion of consumer trust. Instead, they verify their own insurance in advance to access guaranteed, upfront prices. They then browse doctors and treatments, book directly to the practice’s EHR, pay upfront, and complete intake in their native languages before arriving for the appointment.
Administrators instantly verify eligibility and covered services, schedule multi-visit encounters in under 30 seconds, update visit costs in real-time as emergent treatments are rendered, and collect payment all in one tool. This model guarantees consumer cost-shares are paid before the claims cycle begins.
Ultimately, Superscript’s intervention brings healthcare in line with standard market behaviors in consumer facing categories. Consumers are empowered to make informed choices about where they seek care. Practices are empowered to focus on differentiation by providing the best care, and the best experience.
Jamie Hajee Sheriff
- MRN ID to match patient charts
- Insurance verified upfront
- Real-time eligibility checks on demand
- Schedule with real-time availability
- See self-pay & insured cost shares
- Collect payment & digital intake
Existing views of upcoming and past appointments show details relevant to scheduling. Context on payment and pricing aren’t available in a synthesized view. Payment collection is not easily accessible.
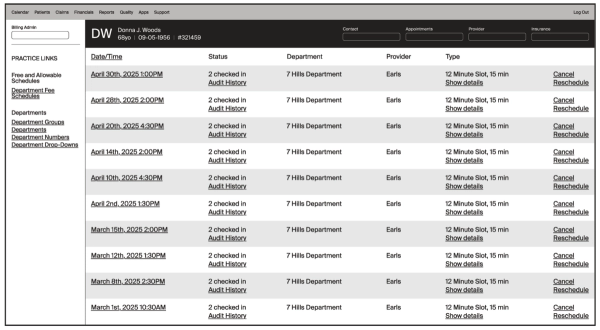
EHRs reflect the patchwork of steps necessary to coordinate patient care. These softwares house necessary information, but fail to synthesize it effectively. Their core functionalities are not optimized to meet the needs of their primary users. The consequences are time-consuming and tedious workflows.
Existing views of upcoming and past appointments show details relevant to scheduling. Context on payment and pricing aren’t available in a synthesized view. Payment collection is not easily accessible.
EHRs reflect the patchwork of steps necessary to coordinate patient care. These softwares house necessary information, but fail to synthesize it effectively. Their core functionalities are not optimized to meet the needs of their primary users. The consequences are time-consuming and tedious workflows.
All appointment context is available in one view. Slots include insurance status, upfront prices, and the applied benefit. Verified, priced appointments are created in under 30 seconds. In one click, navigate to intake forms and payment collection. View all requisite patient information, and all services rendered in an appointment.
Donna J. Woods
All healthcare journeys have three prerequisite steps: scheduling, payment, and intake. Leveraging one tool to facilitate all three simplifies the process, and enables an elegant experience for practices and consumers.
All appointment context is available in one view. Slots include insurance status, upfront prices, and the applied benefit. Verified, priced appointments are created in under 30 seconds. In one click, navigate to intake forms and payment collection. View all requisite patient information, and all services rendered in an appointment.
Donna J. Woods
All healthcare journeys have three prerequisite steps: scheduling, payment, and intake. Leveraging one tool to facilitate all three simplifies the process, and enables an elegant experience for practices and consumers.
All Superscript Practices
Five Specialties: Interventional Cardiology, Outpatient Surgery, OBGYN, Pain Management, Mental Health, Longevity
Total Patient Volume: 272,000 Unique Consumers
Integrated EHR Platforms: Athena, eCW
Time in Market: 16 months
With the Practice Companion (PC) alone, Superscript has given nearly 8,000 patients their cost shares upfront. Nearly 60% of those consumers paid ahead of treatment. For 15% of visits intake and payment were both complete before patients arrived in-office, leaving front desk staff one click away from check-in. Throughout the duration of Superscript’s utilization, nearly 12,500 visits have been scheduled, checked in, and paid for.
Superscript’s Storefront delivers the first true e-commerce experience to the industry. Conversion rates for both insured and self-pay Storefronts rival those in the highest performing e-commerce categories. Notably, consumers paying with insurance transacted more often than those in nearly all other industries. What started as a theory about a new model of paying for care has been thoroughly validated.
Superscript’s technology is built to account for the idiosyncrasies of payer rules per practice, per provider with benefit logic mapped across 95% of existing health plans. The system collects and verifies unique benefit types—including in-benefit deductibles, special copays, and visit limitations—with 98.6% accuracy. This occurs both at the point of sale and prior to the consumer’s appointment.
Superscript’s Bester Match package selection outperforms both manual selection and automated EHR selection with 96% accuracy.
The PC serves as a complete operating system for the modern front desk administrator. It effectively centralizes and automates administrative tasks related to patient check-in.
PC Functionalities:
- Appointment Scheduling
- Eligibility & Verification of Benefits
- Pricing Consumer Cost-Shares
- Payment Collection
- Patient Registration & Intake
- Appointment Reminders
- Additional Tests & Services
- Monitoring Live Transfers & Payments
The PC compliments clinical processes carried out in an EHR by extracting pre and post-treatment related actions away from the doctor’s encounter with a patient. At the front desk, Patient Services Representatives leverage one system to accurately verify eligibility and benefits for all patients. Patient demographic information is always up-to-date with smart intake that auto-sends on the year mark. Inactive or Unverified insurances are flagged during schedule review. Consolidating this information and these actions into one tool minimizes room for clerical error. For billing and RCM teams, the steps to prevent claim denials are automated, and complete before patients receive care.
- Patient
- Clarissa Goudeau
- Date
- 09/24/2025
- Claim ID
- 312891
- Transfer Status
- Transferred collected amount
- Amount
- $1,5000
The lack of clarity in engaging with insurance plans previously made avoiding denials a trial and error process. Superscript’s PC automates what EHRs cannot. It learns in real-time and can offer practice’s aggregate, data-driven insights on causes for denial. Where applicable, the tool will adapt and optimize its package and demographics selections to reduce the likelihood of a denial.
With the Practice Companion, Superscript has brought in over $2.6 million in guaranteed patient responsibility. Assuming standard medical debt, this translates to an estimated $501,100 in eliminated bad debt.
The “Live Transfers Table” offers real-time reporting on collections per user, claim status, and recommended actions to ensure collection of consumer responsibility. For practices with facility, anesthesia and physician fees, the PC splits payments and transfers balances to the appropriate recipient.
Case Study 1: Sorin Medical
Specialty: Interventional Cardiology, Outpatient Surgery
Patient Volume: approx. 4,700 / month
Integrated Superscript Products: Storefront, Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: athenaOne
With the addition of the Storefront, Sorin’s new patient volume has grown by over 10%, accounting for roughly a third of all new patients at the practice adding $235,500 in upfront collections. On average, these consumers returned to the practice 2.5 times after their first visit generating over $580,000 in additional lifetime value. Consumers even used the Storefront to purchase Sorin’s trademarked heart scan as gift for loved ones.
In December 2024, Superscript rolled out their intake functionality for Sorin patients. To date, 199 patients have completed intake digitally in 4 languages, saving 23,880 minutes of admin and patient time. Consumers found these experiences highly satisfactory, as they greeted front-desk staff with all recommended steps complete.
“Collaborating with Superscript aligns perfectly with our mission to provide accessible, quality, transparent, and affordable healthcare.” — Dr. Joseph Puma, Founder of Sorin Medical
A press release announcing the partnership goes on to say: “Sorin Medical’s partnership with Superscript underscores our dedication to providing accessible, high-quality, and cost-effective healthcare. We strive to offer solutions that surpass the offerings of major hospital academic centers in the city, both in quality and affordability. Our approach challenges the traditional healthcare model, ensuring that exceptional medical services are accessible to all communities.
This collaboration with Superscript sets a new standard in healthcare, reaffirming Sorin Medical’s role as a pioneer in the industry. By integrating Superscript’s transparent insurance pricing model, we are redefining healthcare affordability and accessibility, making quality care a right for all.”
Case Study 2: Hudson Medical
Specialty: Pain Management
Patient Volume: approx. 2,100 / month
Integrated Superscript Products: Storefront, Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: athenaOne
Hudson Medical increased consumer out-of-pocket collections by 88% with Superscript’s Storefront. 50% of consumers opted to self-schedule when purchasing online. Hudson’s Storefront shows consumers their out-of-pocket responsibility for all possible treatment paths. From consultations to services that may only be prescribed post diagnosis, the Storefront offers consumers cost clarity throughout their journey. Hudson is distinguished amongst pain management clinics for leveraging this feature, a striking competitive edge.
To ensure these tools work harmoniously, the PC and the EHR maintain information parity. Patient demographic information, upcoming and past appointments, and services rendered during a visit are regularly synced across platforms. This ensures successful scheduling and check-in motions on the PC. At Hudson Medical, 97% of the time these actions are completed entirely in the PC.
Superscript’s intake solution deprecated the practice’s reliance on NexHealth. Patient Registration, HIPAA Authorization & Consent, and procedure-specific forms are digitized and auto-sent as soon as an appointment is scheduled. Superscript completes all required fields for patient registration as forms are instantly saved to the patient’s chart. Appointment reminders are sent along with forms at a customized cadence.
Case Study 3: EXTENSION HEALTH
Specialty: Longevity
Patient Volume: approx. 300 / month
Integrated Superscript Products: Storefront, Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: athenaOne
EXTENSION’s marketing campaigns direct consumers to premium services on the Storefront with upfront pricing, treatment details and real-time provider availability. Around events like the Don’t Die Summit in February 2025, up to 49 consumers made purchases on a single day with the Storefront’s seamless payment experience. They self-scheduled appointments directly into the practice’s EHR for treatments that permit consumer scheduling. This e-commerce experience attracts roughly 36 new patients per month. The practice also reported a reduction in no shows and cancellations, as collecting payment upfront, prior to appointments, discourages this behavior.
The Storefront also facilitates payment plans and promotional discounts for self-pay services, a unique opportunity for practices to capture new patients. In-office, Superscript’s bespoke Kiosk Check-In product will allow consumers to self-check-in on arrival at the office. Any outstanding items that are prerequisites to care may be completed at this kiosk without engaging front-desk staff.
As consumers buy healthcare services with full knowledge of treatment and cost, practices can effectively promote service offerings and reduce friction points in care coordination with patients.
Case Study 4: QOGYN
Specialty: OBGYN
Patient Volume: approx. 3,900 / month
Integrated Superscript Products: Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: eCW
In leveraging the PC, QOGYN will reduce the number of unique verification tools from roughly six to one. The PC’s “Active” tab signals a consumer is ready to be seen, deprecating the need for a physical sign-in sheet to manage walk-in and scheduled patients.
QOGYN will pilot Superscript’s interoperability solution for referrals, deprecating the manual work of transferring patient data. The PC ensures information parity across all integrated platforms. That allows the system to recognize existing patient profiles or create new ones as needed. On this foundation, sophisticated actions like inter-EHR scheduling, and selecting the correct insurance package for claim submission, are automated cross-practice.
Scheduling staff at QOGYN will thus utilize the PC to create appointments on specialists’ calendars between Athenaone and distinct eCW instances. All relevant documentation and patient demographics are inputted once, and transferred across integrated EHR systems. The same workflow will be enabled in the reverse when QOGYN’s providers are on-site specialists at satellite Primary Care clinics.
All Superscript Practices
Five Specialties: Interventional Cardiology, Outpatient Surgery, OBGYN, Pain Management, Mental Health, Longevity
Total Patient Volume: 272,000 Unique Consumers
Integrated EHR Platforms: Athena, eCW
Time in Market: 16 months
With the Practice Companion (PC) alone, Superscript has given nearly 8,000 patients their cost shares upfront. Nearly 60% of those consumers paid ahead of treatment. For 15% of visits intake and payment were both complete before patients arrived in-office, leaving front desk staff one click away from check-in. Throughout the duration of Superscript’s utilization, nearly 12,500 visits have been scheduled, checked in, and paid for.
Superscript’s Storefront delivers the first true e-commerce experience to the industry. Conversion rates for both insured and self-pay Storefronts rival those in the highest performing e-commerce categories. Notably, consumers paying with insurance transacted more often than those in nearly all other industries. What started as a theory about a new model of paying for care has been thoroughly validated.
Superscript’s technology is built to account for the idiosyncrasies of payer rules per practice, per provider with benefit logic mapped across 95% of existing health plans. The system collects and verifies unique benefit types—including in-benefit deductibles, special copays, and visit limitations—with 98.6% accuracy. This occurs both at the point of sale and prior to the consumer’s appointment.
Superscript’s Bester Match package selection outperforms both manual selection and automated EHR selection with 96% accuracy.
The PC serves as a complete operating system for the modern front desk administrator. It effectively centralizes and automates administrative tasks related to patient check-in.
PC Functionalities:
- Appointment Scheduling
- Eligibility & Verification of Benefits
- Pricing Consumer Cost-Shares
- Payment Collection
- Patient Registration & Intake
- Appointment Reminders
- Additional Tests & Services
- Monitoring Live Transfers & Payments
The PC compliments clinical processes carried out in an EHR by extracting pre and post-treatment related actions away from the doctor’s encounter with a patient. At the front desk, Patient Services Representatives leverage one system to accurately verify eligibility and benefits for all patients. Patient demographic information is always up-to-date with smart intake that auto-sends on the year mark. Inactive or Unverified insurances are flagged during schedule review. Consolidating this information and these actions into one tool minimizes room for clerical error. For billing and RCM teams, the steps to prevent claim denials are automated, and complete before patients receive care.
- Patient
- Clarissa Goudeau
- Date
- 09/24/2025
- Claim ID
- 312891
- Transfer Status
- Transferred collected amount
- Amount
- $1,5000
The lack of clarity in engaging with insurance plans previously made avoiding denials a trial and error process. Superscript’s PC automates what EHRs cannot. It learns in real-time and can offer practice’s aggregate, data-driven insights on causes for denial. Where applicable, the tool will adapt and optimize its package and demographics selections to reduce the likelihood of a denial.
With the Practice Companion, Superscript has brought in over $2.6 million in guaranteed patient responsibility. Assuming standard medical debt, this translates to an estimated $501,100 in eliminated bad debt.
The “Live Transfers Table” offers real-time reporting on collections per user, claim status, and recommended actions to ensure collection of consumer responsibility. For practices with facility, anesthesia and physician fees, the PC splits payments and transfers balances to the appropriate recipient.
Case Study 1: Sorin Medical
Specialty: Interventional Cardiology, Outpatient Surgery
Patient Volume: approx. 4,700 / month
Integrated Superscript Products: Storefront, Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: athenaOne
With the addition of the Storefront, Sorin’s new patient volume has grown by over 10%, accounting for roughly a third of all new patients at the practice adding $235,500 in upfront collections. On average, these consumers returned to the practice 2.5 times after their first visit generating over $580,000 in additional lifetime value. Consumers even used the Storefront to purchase Sorin’s trademarked heart scan as gift for loved ones.
In December 2024, Superscript rolled out their intake functionality for Sorin patients. To date, 199 patients have completed intake digitally in 4 languages, saving 23,880 minutes of admin and patient time. Consumers found these experiences highly satisfactory, as they greeted front-desk staff with all recommended steps complete.
“Collaborating with Superscript aligns perfectly with our mission to provide accessible, quality, transparent, and affordable healthcare.” — Dr. Joseph Puma, Founder of Sorin Medical
A press release announcing the partnership goes on to say: “Sorin Medical’s partnership with Superscript underscores our dedication to providing accessible, high-quality, and cost-effective healthcare. We strive to offer solutions that surpass the offerings of major hospital academic centers in the city, both in quality and affordability. Our approach challenges the traditional healthcare model, ensuring that exceptional medical services are accessible to all communities.
This collaboration with Superscript sets a new standard in healthcare, reaffirming Sorin Medical’s role as a pioneer in the industry. By integrating Superscript’s transparent insurance pricing model, we are redefining healthcare affordability and accessibility, making quality care a right for all.”
Case Study 2: Hudson Medical
Specialty: Pain Management
Patient Volume: approx. 2,100 / month
Integrated Superscript Products: Storefront, Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: athenaOne
Hudson Medical increased consumer out-of-pocket collections by 88% with Superscript’s Storefront. 50% of consumers opted to self-schedule when purchasing online. Hudson’s Storefront shows consumers their out-of-pocket responsibility for all possible treatment paths. From consultations to services that may only be prescribed post diagnosis, the Storefront offers consumers cost clarity throughout their journey. Hudson is distinguished amongst pain management clinics for leveraging this feature, a striking competitive edge.
To ensure these tools work harmoniously, the PC and the EHR maintain information parity. Patient demographic information, upcoming and past appointments, and services rendered during a visit are regularly synced across platforms. This ensures successful scheduling and check-in motions on the PC. At Hudson Medical, 97% of the time these actions are completed entirely in the PC.
Superscript’s intake solution deprecated the practice’s reliance on NexHealth. Patient Registration, HIPAA Authorization & Consent, and procedure-specific forms are digitized and auto-sent as soon as an appointment is scheduled. Superscript completes all required fields for patient registration as forms are instantly saved to the patient’s chart. Appointment reminders are sent along with forms at a customized cadence.
Case Study 3: EXTENSION HEALTH
Specialty: Longevity
Patient Volume: approx. 300 / month
Integrated Superscript Products: Storefront, Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: athenaOne
EXTENSION’s marketing campaigns direct consumers to premium services on the Storefront with upfront pricing, treatment details and real-time provider availability. Around events like the Don’t Die Summit in February 2025, up to 49 consumers made purchases on a single day with the Storefront’s seamless payment experience. They self-scheduled appointments directly into the practice’s EHR for treatments that permit consumer scheduling. This e-commerce experience attracts roughly 36 new patients per month. The practice also reported a reduction in no shows and cancellations, as collecting payment upfront, prior to appointments, discourages this behavior.
The Storefront also facilitates payment plans and promotional discounts for self-pay services, a unique opportunity for practices to capture new patients. In-office, Superscript’s bespoke Kiosk Check-In product will allow consumers to self-check-in on arrival at the office. Any outstanding items that are prerequisites to care may be completed at this kiosk without engaging front-desk staff.
As consumers buy healthcare services with full knowledge of treatment and cost, practices can effectively promote service offerings and reduce friction points in care coordination with patients.
Case Study 4: QOGYN
Specialty: OBGYN
Patient Volume: approx. 3,900 / month
Integrated Superscript Products: Practice Companion (PC)
Payment Methods: Self-Pay, Insurance
EHR: eCW
In leveraging the PC, QOGYN will reduce the number of unique verification tools from roughly six to one. The PC’s “Active” tab signals a consumer is ready to be seen, deprecating the need for a physical sign-in sheet to manage walk-in and scheduled patients.
QOGYN will pilot Superscript’s interoperability solution for referrals, deprecating the manual work of transferring patient data. The PC ensures information parity across all integrated platforms. That allows the system to recognize existing patient profiles or create new ones as needed. On this foundation, sophisticated actions like inter-EHR scheduling, and selecting the correct insurance package for claim submission, are automated cross-practice.
Scheduling staff at QOGYN will thus utilize the PC to create appointments on specialists’ calendars between Athenaone and distinct eCW instances. All relevant documentation and patient demographics are inputted once, and transferred across integrated EHR systems. The same workflow will be enabled in the reverse when QOGYN’s providers are on-site specialists at satellite Primary Care clinics.
Practices and consumers are demonstrably marginalized by healthcare’s status quo. As it exists today, it is wasteful, convoluted, and its value is diluted by incentive structures that steer it away from its purpose. The complexity and uncertainty associated with billing and paying for care diverts resources away from providing it. Private practice is prohibitively expensive to young physicians, and consumers are discouraged from seeking care when they need it. The lack of interoperability is time-consuming and ineffectual. It restricts certain tasks to manual completion on paper. Standard solutions force practices to adopt a patchwork of software platforms, ultimately compounding the issue of siloed data and information. Bills that appear weeks after treatment are readily dismissed by disgruntled consumers. Providers are forced to spend more time and resources in EHRs than they are with patients.
Fixing healthcare is a formidable challenge. Superscript’s co-founders, Ritayan Chakraborty and Rahul Naidoo, are clear about the role they play. “No one company can fix U.S. healthcare,” Chakraborty explains, “but consumers can, if they’re empowered to use it effectively. That’s where we come in.”
Superscript translates healthcare into digital experiences that consumers understand. Its solutions empower a vanguard of clinicians and administrators to shepherd healthcare through its consumer evolution. Why? It provides information and clarity enabling a radically different healthcare journey to those providing and receiving care. Improving the consumer experience is only possible by improving the experience for providers too. Solving the intractable problems that weigh this industry down is a prerequisite to heralding systemic change. Superscript is healthcare’s connective tissue, building whatever is necessary to bring simplicity, trust, and transparency to all of healthcare.
References
- Congressional Budget Office. (2024, March). The budget and economic outlook: 2024 to 2034.
- Calculated with 2023 total GDP. ($735 billion/$27.36 trillion) * 100 = 2.68%
- Tseng, P., Kaplan, R. S., Richman, B. D., Shah, M. A., & Schulman, K. A. (2018). Administrative costs associated with physician billing and insurance-related activities at an academic health care system. JAMA, 319(7), 691–697.
- Himmelstein, D. U., Jun, M., Busse, R., Chevreul, K., Geissler, A., Jeurissen, P., ... & Woolhandler, S. (2009). A comparison of hospital administrative costs in eight nations: U.S. costs exceed all others by far. Health Affairs, 28(4), w544–w554.
- Medical Billing & Management Services. (2024, February 12). Patient collection rate falls to nearly 50 percent.
- American Medical Association. (2024). Medicare physician payment updates compared to inflation, 2001–2025.
- Tolbert, J., & Semanskee, A. (2023, December 14). Standardized plans in the health care marketplace: Changing requirements and increasing options. KFF. NOTE: Plans listed on HealthCare.gov do not include employer-sponsored plans or the comprehensive set of Medicare and Medicaid plans.
- Tolbert, J., & Long, M. (2024, March 20). Consumer survey highlights problems with denied health insurance claims. KFF.
- Premier Inc. (2024, March 21). Trend alert: Private payers retain profits by refusing or delaying legitimate medical claims.
- NORC at the University of Chicago. (2022, August 10). New survey reveals 57% of Americans have been surprised by a medical bill.
- Centers for Medicare & Medicaid Services. NHE fact sheet. U.S. Department of Health and Human Services.
- Sarnak, D. O., & Amin, K. (2023, October 12). High U.S. health care spending: Where is it all going? The Commonwealth Fund.
- Gee, E., & Spiro, T. (2021, March 16). Excess administrative costs burden the U.S. health care system. Center for American Progress.
- Sarnak, et al. (2023, October 12). See citation 12.
- Ornstein, C., & Jones, R. G. (2024, February 1). How often do health insurers deny patients’ claims? ProPublica.
- Gee, et al. (2019). See citation 13.
- Sorin Medical. (2023, December 11). Sorin Medical and Superscript unveil groundbreaking partnership for healthcare pricing transparency.
Practices and consumers are demonstrably marginalized by healthcare’s status quo. As it exists today, it is wasteful, convoluted, and its value is diluted by incentive structures that steer it away from its purpose. The complexity and uncertainty associated with billing and paying for care diverts resources away from providing it. Private practice is prohibitively expensive to young physicians, and consumers are discouraged from seeking care when they need it. The lack of interoperability is time-consuming and ineffectual. It restricts certain tasks to manual completion on paper. Standard solutions force practices to adopt a patchwork of software platforms, ultimately compounding the issue of siloed data and information. Bills that appear weeks after treatment are readily dismissed by disgruntled consumers. Providers are forced to spend more time and resources in EHRs than they are with patients.
Fixing healthcare is a formidable challenge. Superscript’s co-founders, Ritayan Chakraborty and Rahul Naidoo, are clear about the role they play. “No one company can fix U.S. healthcare,” Chakraborty explains, “but consumers can, if they’re empowered to use it effectively. That’s where we come in.”
Superscript translates healthcare into digital experiences that consumers understand. Its solutions empower a vanguard of clinicians and administrators to shepherd healthcare through its consumer evolution. Why? It provides information and clarity enabling a radically different healthcare journey to those providing and receiving care. Improving the consumer experience is only possible by improving the experience for providers too. Solving the intractable problems that weigh this industry down is a prerequisite to heralding systemic change. Superscript is healthcare’s connective tissue, building whatever is necessary to bring simplicity, trust, and transparency to all of healthcare.
References
- Congressional Budget Office. (2024, March). The budget and economic outlook: 2024 to 2034.
- Calculated with 2023 total GDP. ($735 billion/$27.36 trillion) * 100 = 2.68%
- Tseng, P., Kaplan, R. S., Richman, B. D., Shah, M. A., & Schulman, K. A. (2018). Administrative costs associated with physician billing and insurance-related activities at an academic health care system. JAMA, 319(7), 691–697.
- Himmelstein, D. U., Jun, M., Busse, R., Chevreul, K., Geissler, A., Jeurissen, P., ... & Woolhandler, S. (2009). A comparison of hospital administrative costs in eight nations: U.S. costs exceed all others by far. Health Affairs, 28(4), w544–w554.
- Medical Billing & Management Services. (2024, February 12). Patient collection rate falls to nearly 50 percent.
- American Medical Association. (2024). Medicare physician payment updates compared to inflation, 2001–2025.
- Tolbert, J., & Semanskee, A. (2023, December 14). Standardized plans in the health care marketplace: Changing requirements and increasing options. KFF. NOTE: Plans listed on HealthCare.gov do not include employer-sponsored plans or the comprehensive set of Medicare and Medicaid plans.
- Tolbert, J., & Long, M. (2024, March 20). Consumer survey highlights problems with denied health insurance claims. KFF.
- Premier Inc. (2024, March 21). Trend alert: Private payers retain profits by refusing or delaying legitimate medical claims.
- NORC at the University of Chicago. (2022, August 10). New survey reveals 57% of Americans have been surprised by a medical bill.
- Centers for Medicare & Medicaid Services. NHE fact sheet. U.S. Department of Health and Human Services.
- Sarnak, D. O., & Amin, K. (2023, October 12). High U.S. health care spending: Where is it all going? The Commonwealth Fund.
- Gee, E., & Spiro, T. (2021, March 16). Excess administrative costs burden the U.S. health care system. Center for American Progress.
- Sarnak, et al. (2023, October 12). See citation 12.
- Ornstein, C., & Jones, R. G. (2024, February 1). How often do health insurers deny patients’ claims? ProPublica.
- Gee, et al. (2019). See citation 13.
- Sorin Medical. (2023, December 11). Sorin Medical and Superscript unveil groundbreaking partnership for healthcare pricing transparency.